FDA commissioner starts pushing Pfizer drugs - A huge breach of ethics | Dr. Vinay Prasad
Dr. Vinay Prasad discusses a recent Twitter thread by FDA commissioner dr. Robert Califf in which Califf promotes Pfizer's highly profitable drug Paxlovid and also highly profitable COVID and flu vaccination.
The first important point is that both the experimental jabs and other experimental medications such as Paxlovid and Molnupiravir, were only granted Emergency Use Authorization (EUA). Since there is no emergency at this time, the EUA should be immediately retracted, making it illegal to market these highly profitable products. Instead, the 'emergency' keeps being extended allowing more wealth transferal to the pharmaceutical companies.
"The FDA protects the big drug companies, and is subsequently rewarded, and using the government's police powers, they attack those who threaten the big drug companies. People think that the FDA is protecting them. It isn't. What the FDA is doing, and what the public thinks it is doing are as different as night and day."
— Dr. Herbert Ley (1923-2001). Former commissioner of the US FDA. (Made this comment in the year 1969)
Califf distracts the attention from the discussion about the well-known 'rare' Paxlovid rebound where people experience a reduction in symptoms only to get sick again after a few days. Paxlovid seems to be a pause button at best: it doesn't cure you, but only suppresses symptoms for a short time, after which they come back.
Reduction of symptom duration is not very important according to Califf. It's all about reduction in hospitalization and death.
First of all, if the Paxlovid rebound is so rare, how come that so many prominent people (e.g. Walensky, Fauci, Biden) experience this rebound?
Second of all, I agree that the discussion should be about patient centric outcome, among which hospitalization and death are the most important. However, symptom duration is also a patient centric outcome.
NB: Examples of non-patient centric outcomes, are PCR positivity, viral load and antibodies. These are mostly or completely irrelevant.
Califf discusses whether the rebound is due to COVID or due to Paxlovid. News flash: If the rebound only occurs when treated with Paxlovid, it's due to Paxlovid.
Califf mentions that Paxlovid showed a 90% reduction in hospitalization and death in Pfizer's clinical trial. However, he does not mention that the trial was conducted among unvaxxed and that the results cannot be assumed to also be valid among the vaxxed.
He also doesn't mention Randomized Controlled Trials (RCT's) should be called RESULTS Controlled Trials as pharmaceutical companies and their accomplices use every fraud and misleading tactic to present the results that are beneficial to them.
Marcia Angell wrote: "It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine."
Califf doesn't mention the enormous number of severe negative interactions between Paxlovid and other medications. Of course, he also doesn't mention unprofitable alternatives, such as ventilation, vitamin D, a healthier diet and lifestyle, early intensive combination treatment with cheap safe off-label (thus off-profit) products, etc.
Dr. Prasad says, "The most important question is in whom Paxlovid actually has a benefit". I would say the most important question is first of all about better alternatives (see previous paragraph) and second about risk/cost vs benefits.
Dr. Prasad criticizes real-world data as "shitty confounded observational data" due to possible confounders. While this can be true, RCT's are hardly reliable either. This is due to the above mentioned fraud and misleading, but also due to other factors, such as wrong protocols, too little participants, the wrong participants, delay, short observational periods, measuring non patient centric outcomes, etc. etc.
Second of all, it has been shown that large observational studies produce the same results as RCT's. See:
Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.MR000034.pub2/full
👆 "[O]n average, there is little evidence for significant effect estimate differences between observational studies and RCTs, regardless of specific observational study design, heterogeneity, or inclusion of studies of pharmacological interventions."
FDA commissioners usually only start promoting drugs AFTER they've left the FDA and started a very lucrative job at the pharmaceutical companies they were supposed to referee just shortly before. They get this lucrative job as reward for playing nice in their previous function. This phenomenon is the well-known revolving door. Robert Califf seems to be the first to start blatantly promoting highly profitable drugs even while at the FDA.
SEE ALSO
"The FDA would NEVER accept a bribe": Excellent satire of kindergartners getting brainwashed
https://rumble.com/v1elo91
DESCRIPTION BY VINAY PRASAD
Vinay Prasad, MD MPH; Physician & Professor
Hematologist/ Oncologist
Professor of Epidemiology, Biostatistics and Medicine
Author of 450+ Peer Reviewed papers, 2 Books, 2 Podcasts, 100+ op-eds.
If you want to contact me, do it here: http://www.vinayakkprasad.com/contact
Google Scholar: https://scholar.google.com/citations?user=ym4rwk0AAAAJ&hl=en
Substack: https://vinayprasadmdmph.substack.com/
Podcast: https://podcasts.apple.com/us/podcast/plenary-session/id1429998903
Personal Website: www.vinayakkprasad.com
Laboratory Website: www.vkprasadlab.com
Podcast Website: www.plenarysessionpodcast.com
Academic Publications: http://www.vinayakkprasad.com/papers
Follow me on:
Twitter @vprasadmdmph
-
 48:46
48:46
Sunfellow On COVID-19
2 years agoDr. Pierre Kory: Criminal Big Pharma Is "Literally Destroying Society"
9251 -
 13:45
13:45
Asher Press
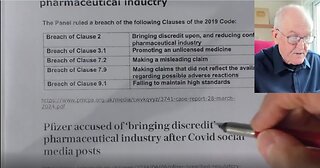
1 month agoPfizer breached regulatory code, watchdog rules; "Pfizer is 'deeply sorry" - Dr John Campbell
220 -
 45:48
45:48
USAFrontlineDoctors
6 months agoDr. James Thorp Reveals Major Corruption Within Pfizer & the Medical Industry
1.34K4 -
 17:52
17:52
Rolling With You
2 months agoDr. John Campbell - Pharmaceutical interests or patient safety
937 -
 1:22:13
1:22:13
Dr. Drew
11 months agoHow Big Pharma Hijacked Evidence-Based Medicine: Dr Aseem Malhotra w/ Dr Kelly Victory – Ask Dr Drew
27.1K35 -
 7:21
7:21
BrigitteNP
2 years agoPfizer FDA APPROVAL COVID-19
66 -
 1:06:25
1:06:25
VACCINE INJURY UPDATES
1 year agoHow Pfizer Bribes Led to Vaccine Mandates
351 -
 23:16
23:16
Sunfellow On COVID-19
2 years agoPro-Vaccine Doctor Discovers He's Been Duped By Pfizer
7.67K43 -
 13:45
13:45
FanaticVoyage
1 month agoPfizer Guilty by UK Watchdog - Letter Is Not Issued By Any Court of Law So Legally Speaking....
136 -
 4:32
4:32
oversea2022
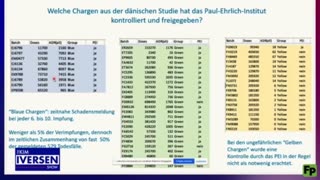
10 months ago"CRIMINAL": Study shows 1 in 3 Pfizer batches likely PLACEBO, regulators likely KNEW
2164